18 Jun

What Is Gynecomastia And How To Avoid It?

1. Introduction
It may seem comical, but the biggest fear for someone using pharmacology is not having heart or kidney problems, it is having female breasts as a man.
This fear often becomes a reality in pharmacology users who aimed for an aesthetic physique but ended up with a mediocre physique and a very unattractive appearance due to the development of gynecomastia.
Today we will see what this phenomenon is, why it occurs, how it is generated, what type of substances can cause its appearance, if we can reverse it, what we can modify in the cycle to prevent it, and if it is permanent and irreversible, what types of surgeries are available, and what they consist of.
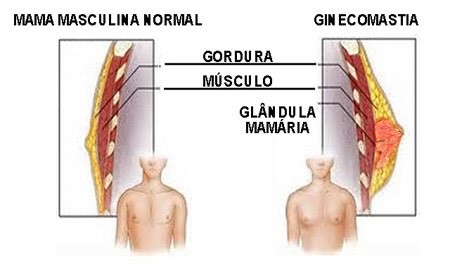
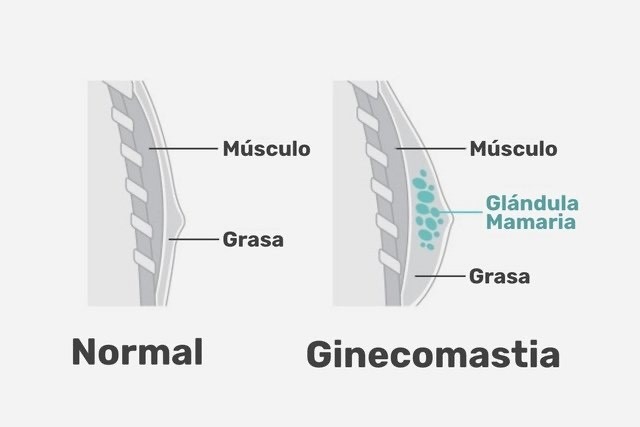
2. What Is Gynecomastia?
Gynecomastia is considered the overdevelopment of the male mammary gland, derived from the use of drugs or of natural origin, but generally has a series of important aesthetic and psychological consequences since literally, it is a female secondary attribute or character and men should not have their chest in that way.
Gynecomastia as such, once installed, is fibrous tissue in the mammary gland, a portion of the chest that the woman normally has very developed, as it is prepared to serve in the future to diffuse breast milk through the mammary ducts and thus feed newborn babies and that obviously in the case of men, this gland should not increase in size since it has no use whatsoever, frequently giving a feminine appearance that does not help at all.
Gynecomastia can be caused by a variety of factors, such as hormonal changes, use of certain medications, underlying medical conditions, or genetics.
It can affect men of all ages and often causes physical and emotional discomfort. In some cases, it may disappear on its own, but in other cases, it may require medical or surgical treatment, depending on the cause and severity of the gynecomastia.
How can it appear naturally, you may wonder... Well, yes, there are several scenarios, and one of them is obesity. It doesn't even have to be morbid obesity, but a significant excess of fat in the body is known to be contrary to optimal hormonal balance.
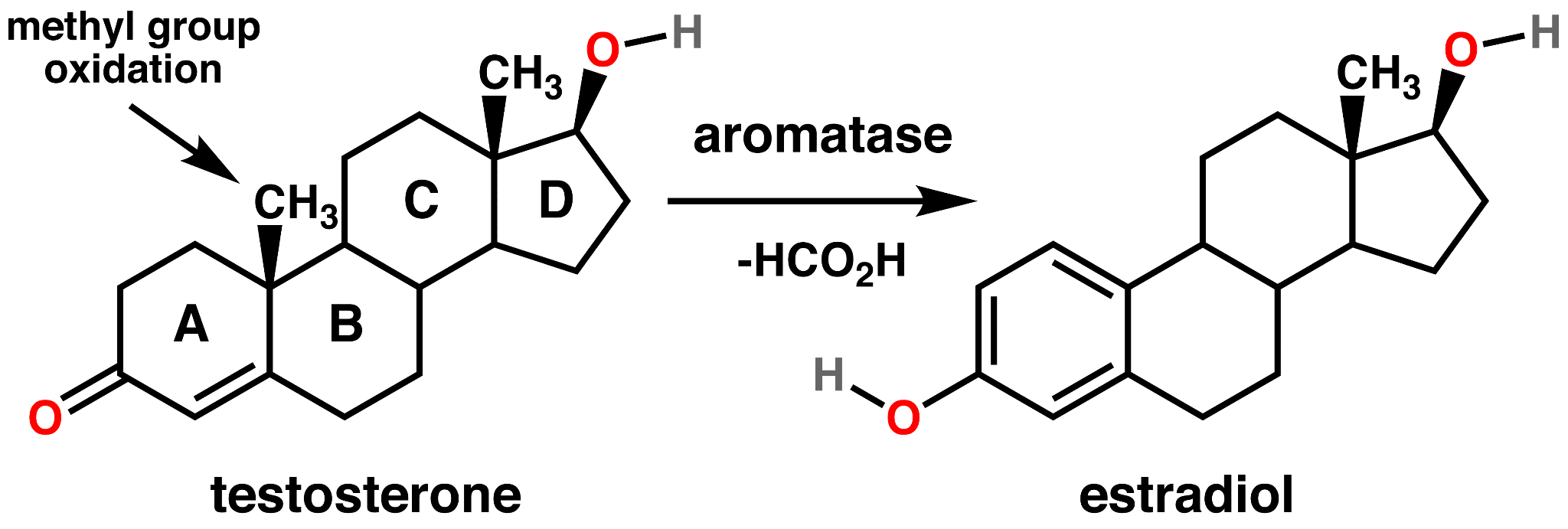
A high body fat percentage increases the activity of the enzyme Alpha Aromatase, which converts testosterone into estradiol, thus raising estrogen levels.
3. How is gynecomastia generated?
What happens in the mammary tissue during the formation of gynecomastia?
Estrogen receptors are distributed in many tissues of the human body and differentiate into two:
(Alpha and estrogen receptor)
-Alpha estrogen receptors
-Beta estrogen receptors
These are present in tissues such as the kidney, heart, brain, lung, adrenal glands, and where it interests us most, in mammary tissue, where the alpha estrogen receptor is located and can generate interaction.
It is important to emphasize that for this process of mammary gland growth to occur, two premises must be met, together or separately:
-Elevation of Estradiol above 10-40pg/ml
-Elevation of Prolactin above 20ng/ml
Can these analytical values be above and not develop the condition of gynecomastia? Yes, absolutely.
The distribution of receptors and the activity of aromatase enzymes and its alpha and beta subunits are genetic, and it is known that people who have been obese or have a family history of obesity have higher enzyme activity or greater sensitivity.
First, there begins to be sensitivity in the nipples, pain, and swelling in that area to the touch, it is the first symptom that an incipient gynecomastia is occurring, but rest assured, even if it is happening, there is a way back, we will see it later.
The problem arises when enough time passes and the mammary gland develops fibrosis, meaning it basically hardens and becomes permanent. Here, surgery is the only solution, with an approximate timeframe of about 6 months.
We'll leave the topic of surgery to the end of the article.
3.1. Natural Causes
As we've discussed, gynecomastia has different origins, and not all of them are pharmacological. Some can be natural due to reasons such as obesity, especially if this obesity occurs during puberty when the hormonal system is developing, and this overactivation of the aromatase enzyme generates an excess of estrogen.
Another reason could simply be a deficit of DHT or Dihydrotestosterone, which doesn't allow for the normal development of the hormonal system and leaves more free estrogen. This is often referred to as "Pubertal Gynecomastia" or "Pseudogynecomastia," and frequently disappears on its own. However, other times, it persists into adulthood.
3.2. Gynecomastia And Steroids
The main reason why an adult man, and probably why you are reading this article, is due to the appearance of gynecomastia from the use of anabolic steroids and derivatives.
This has several reasons, but the main one is an excess of estradiol. It doesn't necessarily have to be the result of aromatization; some anabolic steroids stimulate the production of estradiol without the need to aromatize, and this is an important point because the choice of compounds and the structure of the cycle becomes very relevant.
4. What Steroids Can Cause Gynecomastia?
We could say that all steroids can cause gynecomastia, but that's not true. Some of them do not have the ability to aromatize or interact with the estrogen receptor to elevate estradiol, so they are not capable of causing it.
-The first of them is Testosterone. Yes, we always talk about it as the best of steroids in a generalized way, but it's important to remember that a part of it aromatizes into estradiol, and not all people have the same activity of the Aromatase enzyme. Some people with 750mg will not have symptoms of gynecomastia, and others with 300mg of Testosterone weekly will be enough for it to occur.

-The second are two orals, oxymetholone and dianabol, I put them together because the mechanism by which they elevate estrogens is the same: interaction with estrogen receptors at a systemic level (throughout the body). They also interact with a type of estrogen, methyl-estradiol, which is very difficult to control even with typical drugs that can prevent gynecomastia in general.
-Nandrolone, Trenbolone, and Trestolone: These three compounds belong to the family of 19-Nor Testosterones, a type of steroid considered Nandrolones, which interact in a triple manner, through androgen, estrogen, and progesterone receptors. They have the particularity of not only aromatizing in the case of Nandrolone but also elevating Estradiol through their interaction.
-HCG: It's not a steroid; it's a gonadotropin, a mimic of Luteinizing Hormone. However, this doesn't mean it can't aromatize, not by itself but thanks to the elevations it makes of Testosterone via LH elevation. It should be clarified that low, well-distributed doses of this product don't do it, but when very high doses are used or combined with other drugs that have the ability to aromatize or elevate estrogens as mentioned above, it can occur, and it's important to mention it.
It should be clarified that with low, evenly distributed doses of this product, it doesn't happen, but when very high doses are used or combined with other drugs that have the ability to aromatize or elevate estrogen levels, as mentioned earlier, it can occur, and it's important to mention it.
5. Can Gynecomastia Be Prevented?
Without a doubt, it can be prevented.
1 in every 3 pharmacology users will suffer or has suffered from gynecomastia to some extent, so it's quite common, and the solution isn't always to include tamoxifen or an aromatase inhibitor.
The first of all is to structure a cycle correctly, avoiding above all:
-Orals like Oxymetholone and Dianabol
-Nandrolones like Trenbolone, Trestolone, and Nandrolone in any of its esters
-Very high doses of Testosterone (Individual response)
-High doses or injections of a large amount of HCG (+5000UI)
If we think about a successful drug to prevent gynecomastia, it would undoubtedly be Tamoxifen. Other SERMs like Clomiphene and Raloxifene could be useful, but undoubtedly the choice and the most successful is Tamoxifen.
Tamoxifen is a drug that interacts by selectively inhibiting estrogen receptors in the mammary glands, not in the rest of the tissues, which could have some undesirable health effects that we don't want.
What's the dosage? Well, here's a big parenthesis, as it can be used preventively with 10mg being sufficient. If the individual has a history of obesity or it is already known that it is enough, the dosage can be increased to 20mg. But it should be noted that SERMs generate long-term ophthalmopathies, and if this drug can be dispensed with, it's better. Later I'll explain how.
The maximum dose of Tamoxifen is 60mg; beyond that, it doesn't make sense to use it.
The other group of drugs used are Aromatase Inhibitors, well known as Anastrozole, Exemestane, Letrozole, and these do inhibit the enzyme in a systemic way, not selectively. Therefore, they have more drawbacks, such as reducing estradiol excessively, which may lead to libido and erection problems, which is undesirable.
The dosage of each of these drugs is individual, but I do not advise it as the first line of action, but as a quick remedy to stop the incipient gynecomastia.
If I had to have an action protocol for prevention, it would be like this:
-Eliminate any steroid that can aromatize or elevate estrogen levels
-Reduce Testosterone to 250mg/week
-Include Tamoxifen 10/20mg per day
This would be in case there is no gynecomastia, but you want to ensure that it won't occur during the cycle's development. This protocol isn't necessary.
But if we're talking about the presence of sensitivity, if gynecomastia has appeared to some extent recently and you want to reverse it:
-Eliminate any steroid that can aromatize or elevate estrogen levels
-Reduce Testosterone to 125mg/week
-Include Tamoxifen 20/40mg per day
-Add 12.5mg of Exemestane per day, with a meal
This protocol makes no sense if gynecomastia has been present for more than 6 months, and in some cases, if it's less than 3-4 months, it wouldn't be possible to reverse it, although most of its size could be reduced.
These two action protocols are for prevention and reversal, but they are not the only ones. In fact, now I'm going to explain how to make modifications to your pharmacological therapy so that you don't have to include these drugs, and in most cases, not even reduce Testosterone.
6. Cycle Modifications
Forget about the previous protocols, as we can save these substances if we do this part correctly, which is cycle modifications.
There's a term that I haven't mentioned yet, which is the cherry on top of this cake, which is the A/E balance, between Androgens and estrogens.
Androgens behave in an interesting way; the higher their quantity, the more they displace the enzymatic activity of aromatase. That is, the more we balance the cycle towards purely androgenic, the fewer estrogens.
Attention, an excess of androgens and few estrogens can also have health consequences such as erectile dysfunction and low libido, but this has a simple solution: monitoring through blood tests.
We're interested in several values:
-Free Testosterone
-DHT
-Ultrasensitive Estradiol
-Prolactin
With these values, especially focusing on the estradiol level, we can know where we stand within the cycle and where we should aim for balance. It's important to note that DHT derivatives are not monitorable, so even if we add, for example, Mesterolone or Proviron, it won't show up in the blood test.
We'll specifically use 3 compounds to balance our cycle and reduce estradiol if it's high in the blood tests.
Now I'll give you simple modifications, which should be done one by one, not all at once or in large doses of these.
-Add Mesterolone or Proviron 25-50 mg/day.
Mesterolone is methylated DHT, practically pure DHT that will reduce the circulating estrogen levels.
-Include or increase Primobolan or Methenolone by 100-200mg.
Primobolan is a derivative of DHT with moderate androgenic potency, which will also have the same effect.
In case estradiol is very high and there is already sensitivity, then we can take both actions: even add 100mg of Mesterolone directly or reduce the weekly Testosterone amount simultaneously. What we aim for is a drastic reduction of estradiol.
It's important to understand that there's no written rule about what should be done, but undoubtedly these intra-cycle modifications work very well, and the good thing is that they are monitorable.
If I had to choose one of the many options I've given you, I would say:
-Do at least one cycle of Testosterone alone to assess your response and at what dose you start to feel some sensitivity. At that point, add 10-20mg of Tamoxifen along with 50mg of Mesterolone.
-Now you know the point of aromatization; in the next cycles, don't reach that amount of Testosterone unless it's combined with Primobolan or you've previously added Mesterolone.
If, unfortunately, gynecomastia has been present for more than 6 months, then we move on to the next section and the end of this article.
7. Gynecomastia Surgeries And Their Types
If gynecomastia is already present and is fibrous tissue, then the solution is to undergo surgery.

There are several types of surgery to treat gynecomastia, ranging from minimally invasive procedures to more extensive surgeries. Some common options include:
-Liposuction: This procedure is mainly used when gynecomastia is primarily caused by excess adipose tissue rather than an increase in glandular breast tissue. During liposuction, small cannulas are inserted through small incisions to suction out the excess fat from the chest area.
-Subcutaneous mastectomy: In this procedure, an incision is made around the areola to access the excess glandular tissue. The excess breast tissue is surgically removed, and in some cases, liposuction may also be performed to remove additional fat.
-Total mastectomy: This surgery involves the complete removal of the glandular breast tissue, as well as any excess skin in the chest area. It is more commonly used in cases of severe gynecomastia or when there is significant excess skin. This would be the case for someone who has a strong tendency to gynecomastia and does not want it to reappear since without the gland, it's not possible for it to reappear.
-Areola reduction surgery: In some cases, gynecomastia may be accompanied by enlargement of the areolas. In these cases, surgery can be performed to reduce the size of the areolas and reposition them more aesthetically.
-Breast lift surgery: When there is significant excess skin in the chest area, especially after weight loss, a breast lift surgery may be necessary to reshape and lift the chest.
It's important to assess which is the right option, and in this case, I recommend consulting with your cosmetic surgeon; don't skimp on it because it's something that will accompany you for the rest of your life.
The average price of this intervention is around €3000-€4000; most of the expenses come from the operating room itself, and usually, local anesthesia is used.
I hope you liked it, that it answered some questions you had, and that you can continue your learning in future articles.
Nutribuilder
Julio
PEDs Educator and Bodybuilding Contest Coach